IS OBESITY SURGERY FOR YOU?
WHAT ARE THE BENEFIT OF WEIGHT LOSS SURGERY?
WHAT IS LAPAROSCOPIC SLEEVE GASTRECTOMY (LSG)?
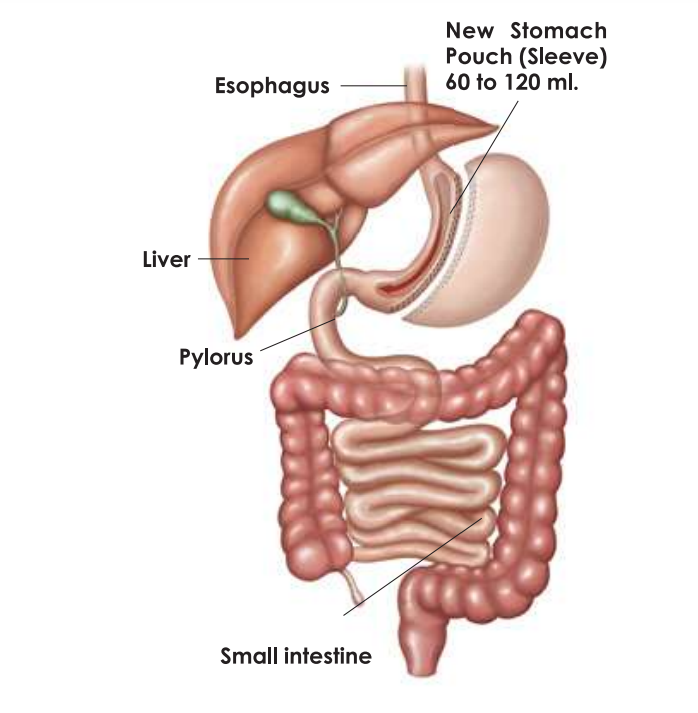
Also called a vertical sleeve gastrectomy or stomach stapling, it is a restrictive procedure. In this procedure the stomach is divided vertically to create a sleeved stomach of the size and shape of a banana. About 80% of the stomach, including the fundus and the left portion of the stomach is removed. The new stomach measures about 60 to 120 ml. The nerves to the stomach and the outlet valve (pylorus) remain intact. This smaller stomach can not hold much food and signals early satiety with a small portion size. Fundus is also the source of hunger hormone “Ghrelin”. Removal of fundus reduces the production of this hormone, which may decrease the desire to eat. These factors combined, lead to weight loss. There is a suggestion that a tighter sleeve yeilds better weight loss results than a loose sleeve in the long term. There is no intestinal bypass.
Click here To Watch Video of lap sleeve gastrectomy.


The procedure requires hospitalisation of three days and has replaced adjustable gastric banding and to some extent r-n-y gastric bypass also. |
WHAT IS ROUX-EN-Y GASTRIC BYPASS & HOW DOES IT WORK?
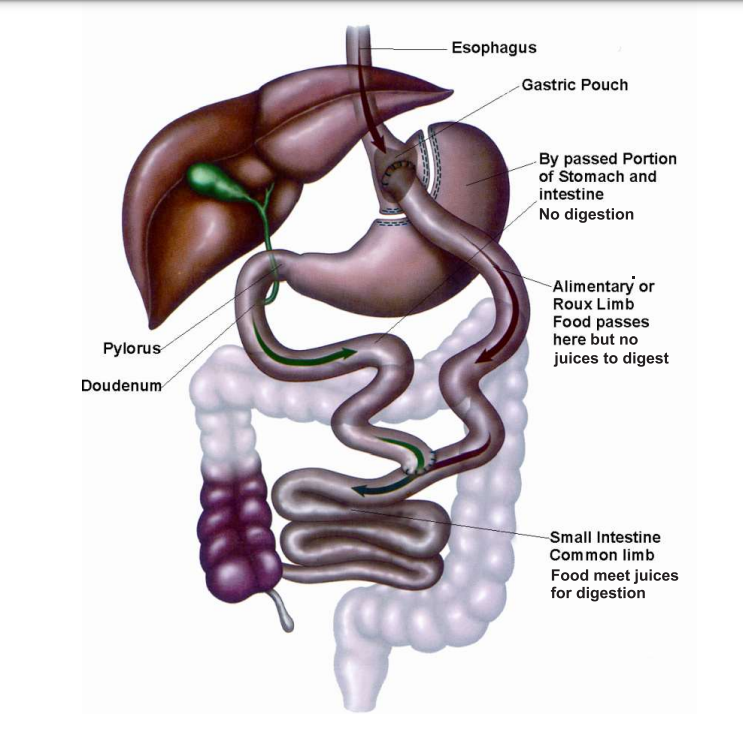
Gastric bypass is a combination of restrictive and malabsorptive procedures. During the surgery, a small Gastric pouch (about 30 ml) is created from the upper part of the stomach using staples. This can hold only a small amount of food. The newly created stomach pouch is then connected directly to the small intestine. The ingested food now bypasses larger part of stomach and a part of small intestine. Patients do not feel hungry, and due to a small stomach pouch, the patient report early sense of fullness and satisfaction and feel full longer. This decreases food intake. Bypassing the stomach and part of intestine means fewer calories are absorbed. Gastric bypass surgery can also lead to changes in gut hormones, which can help improve metabolic health including remission of diabeties type 2.
Click here To Watch Video of Roux-En-Y Gastric Bypass.



The procedure requires hospitalisation of about three days. Supplements of iron, calcium and multi vitamins must be taken regularly to avoid deficiencies.
It is the oldest, the most time tested and studied weight loss procedure, in use for nearly 35 years. It leads to speedier weight loss than other procedures.
It is prompted now for treatment of Diabetes Mellitus Type 2 which is resolved in 84% of patients and often within weeks of surgery.
WHAT IS MINI GASTRIC BYPASS AND HOW DOES IT WORK?
WHAT ARE THE ADVANTAGES OF GASTRIC BYPASS?
HOW TO PREPARE FOR LAPAROSCOPIC WEIGHT LOSS SURGERY?
WHAT TO EXPECT AFTER SURGERY?
WHAT ARE THE RISKS ASSOCIATED WITH WEIGHT LOSS SURGERIES?
WHAT ARE THE LIFE STYLE CHANGES REQUIRED AFTER WEIGHT LOSS SURGERY?
IS OBESITY SURGERY FOR YOU?
WHAT ARE THE BENEFIT OF WEIGHT LOSS SURGERY?
WHAT IS LAPAROSCOPIC SLEEVE GASTRECTOMY (LSG)?
Also called a vertical sleeve gastrectomy or stomach stapling, it is a restrictive procedure. In this procedure the stomach is, divided vertically to create a sleeve (tube) shaped stomach of the size of a banana. About 80% of the stomach, including the fundus and the left portion of the stomach is removed. The new stomach measures about 60 to 120 ml. The nerves to the stomach and the outlet valve (pylorus) remain intact. This smaller stomach can not hold much food and signals early satiety with a small portion size. Fundus is also the source of hunger hormone “Ghrelin”. Removal of fundus reduces the production of this hormone, which may decrease the desire to eat. This factors combined, lead to weight loss. There is a suggestion that a tighter sleeve yeilds better weight loss results than a loose sleeve in the long term. There is no intestinal bypass.
Click here To Watch Video.




The procedure requires hospitalisation of three days and has replaced adjustable gastric banding and to some extent r-n-y gastric bypass also. |
WHAT IS ROUX-EN-Y GASTRIC BYPASS & HOW DOES IT WORK?
Gastric bypass is a combination of restrictive and malabsorptive procedures.
During the surgery, a small Gastric pouch (about 30 ml) is created from the upper part of the stomach using staples. This can hold only a small amount of food. The newly created stomach pouch is then connected directly to the small intestine. and a section of intestine is attached directly to the pouch. The ingested food now bypasses larger part of stomach and a part of small intestine. Patients do not feel hungry, and due to a small stomach pouch, the patient report early sense of fullness and satisfaction and feel full longer. This decreases food intake. Bypassing the stomach and part of intestine means fewer calories are absorbed. Gastric bypass surgery can also lead to changes in gut hormones, which can help improve metabolic health including remission of diabeties type 2.
Click here To Watch Video.


 The procedure requires hospitalisation of about four days.
The procedure requires hospitalisation of about four days.
It is the oldest, the most time tested and studied weight loss procedure, in use for nearly 35 years. It leads speedy weight loss than other procedures. It is the most commonly performed weight loss procedure in the USA.
It is prompted now for treatment of Diabetes Mellitus Type 2 which is resolved in 84% of patients and often within weeks of surgery.