laparoscopic surgeries
Dr. A.K. Kriplani is a nationally recognized leader in the field of laparoscopic surgery. Laparoscopic surgery, often referred to as “keyhole surgery”, is a highly advanced minimally invasive surgical technique, designed for procedures in the abdominal and pelvic regions. This approach utilizes a laparoscope, a slender telescope like instrument equipped with a high-definition camera. The system provides a detailed and magnified view of internal structures on a monitor without the need for extensive incisions. Unlike traditional open surgery, which requires a large 6 to 12 inch incision, laparoscopic procedures involve three to four small punctures, each measuring 5 to 10 millimeter. One cut accommodates the laparoscope for visual guidance, while the others are used for specialized surgical instruments. This innovative technique significantly decreases pain, minimizes recovery time, reduces scarring, and offers a safer alternative for many patients.
Laparoscopic Gallblader Surgery
Gallstones are solid deposits of bile that develop in the gallbladder, often causing pain and digestive issues if untreated.
Scarless Single Incision Laparoscopic Gallblader Surgery
SILS is an innovative technique used for gall bladder removal that offers several advantages over conventional multiport laparoscopy
Laparoscopic Groin Hernia Surgery
An indirect inguinal (Groin) hernia is the most common type, caused by weakness at the internal ring where the testicles descend.
Laparoscopic Ventral Hernia Surgery
Laparoscopic repair offers improved outcome with reduced morbidity by avoiding long incision
Gallbladder
What is Gallbladder ?
HOW DO GALLSTONES FORM?
When the ratio of bile salts, cholesterol and fluid inside the gallbladder becomes unbalanced, some of. the chemicals solidify and form gallstones (a kind of sediment). In majority of patients, cholesterol is the major solid component. While reasons for gallstone formation may be multiple and vary from one person to other, generally:
- Gallstones, are four times more common in females than males.
- Gallstones are more common in females who had pregnancies and are overweight.
- Excess fat in the diet is one of the risk factor.
- Long fasting hours, contraceptive pills, typhoid may be some contributing factors.
However, the cause of gallstone formation may not be apparent. Also no age is exempt and gallstones may form even in a thin, teenager or a child. Our youngest patient was six years old.
What problems Gallstone can produce?
While some gallstones may have no noticeable symptoms, most often they are the cause of pain and other problems.
In the Gallbladder
The stones may be silent, cause pain in upper abdomen lasting for a few hours (biliary colic) with nausea, vomiting, bloating, heartburn and back pain. After many years of irritation, stones may cause cancer of the gallbladder. North India has the highest incidences of gallbladder cancer in the world. Detection of cancer may be difficult in a gallbladder which has become small and contracted. Occasionally after years, stone may erode into the adjacent small intestine (cholecysto duodenal fistula) or large intestine (cholecysto colic fistula) singnificantly increasing morbidity and hospital stay.
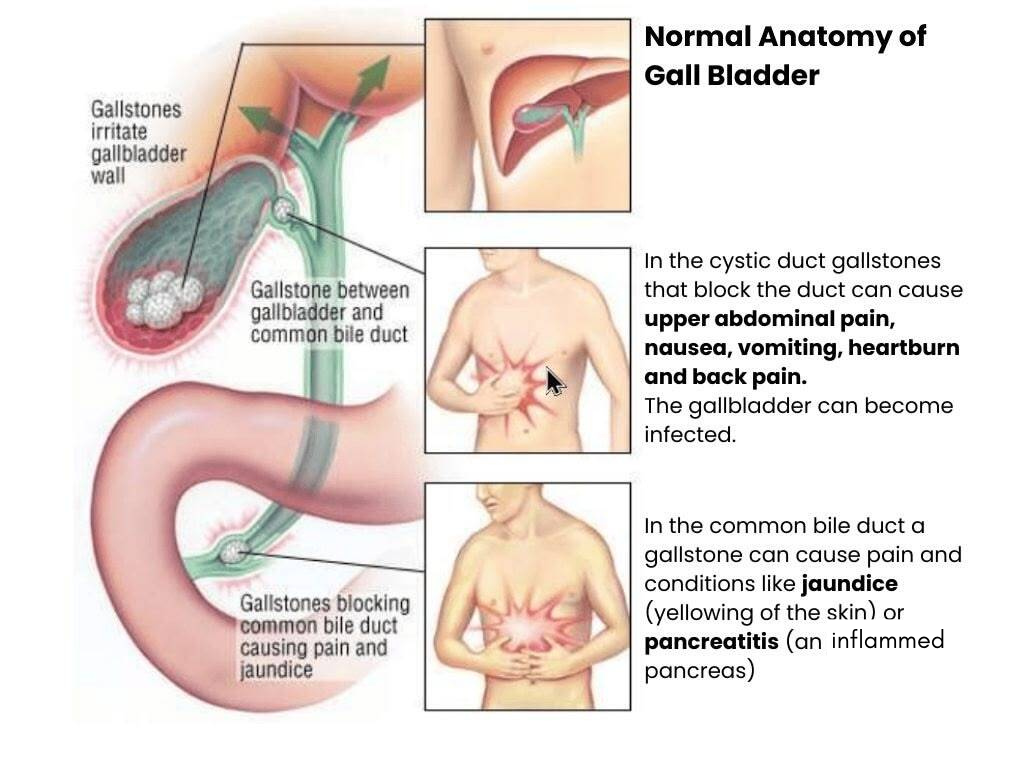
In the Cystic Duct
Gallstones may block the cystic duct causing retention of fluid in the gallbladder (mucocele) or super added infection (acute cholecystitis) resulting in prolonged pain, fever and loss of appetite. Patients having acute cholecystitis need hospitalisation and injectable antibiotics. After treatment, the infection may resolve or lead to pus formation (Empyema). Empyema is more common in patients with diabetes, who are also prone to perforation of gallbladder and leakage of pus (pericholecystic abscess).
In the common bile duct
The stone may move out of the gallbladder through the cystic duct and block the common bile duct. The flow of bile from liver into the intestine gets obstructed and bile gets back into the blood causing jaundice, fever and damage to the liver. Migrating stone may block opening of bile duct into the intestine with swelling of the pancreas (acute pancreatitis) which may require weeks of hospital treatment and may be fatal.
How are Gallstones Treated?
Cholecystectomy: The only effective cure for gallstones
Once stones have formed in the gallbladder, removal of stones with the gallbladder is the only acceptable and effective treatment for permanent cure. Gallstones are formed due to fault in the gallbladder (infection, incomplete emptying, excess water absorption), therefore the gallbladder must be removed. This also eliminates the risk of subsequent cancer developing in the gall bladder. If only stones are removed, the gallbladder will form new stones in the majority of patients. This approach is therefore not accepted. There is no effective medicine to cure gall stones
HOW IS DISEASED GALLBLADDER REMOVED?
The traditional way to remove the diseased gallbladder was through a 15 to 20 cm cut in the abdomen, cutting skin, fat, and three layers of muscles underneath, which were then stitched back in layers (open surgery). Now, the same surgery can be performed through tiny skin punctures, without damaging underlying muscles. The technique is called Laparoscopic cholecystectomy.
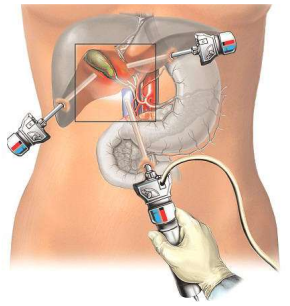
HOW IS LAPAROSCOPIC CHOLECYSTECTOMY PERFORMED?
Commonly, laparoscopic cholecystectomy (lap chole) is performed by four cuts (Multi port Cholecystectomy). These are:
- An 11 mm (1/2 inch) cut in the belly button. Through this port, a telescope is inserted.
- Another 11 mm cut (port) in the upper part of the tummy close to the midline. Through this port instruments are used to dissect the gall bladder free from its attachments and clip the duct and artery of the gall bladder.
- A 6 mm (1/4th inch) cut in the upper part of the tummy on the right side.
- Another 6 mm cut in the right upper abdomen halfway between port no 2 and 3. Through ports number 3 & 4, instruments are used to pull and fix the gall bladder for dissection.
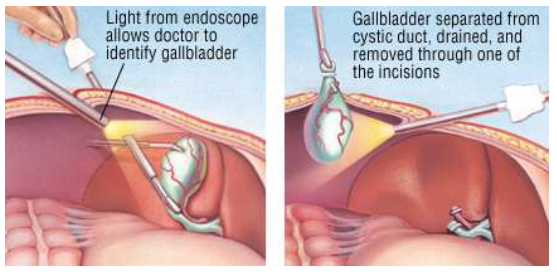
Through the navel, the surgeon inserts a laparoscope which is attached to a lightweight, medical grade video camera. The camera sends images to a monitor, allowing the surgeon and his team to see inside the body. Through other punctures, specially designed instruments are inserted. The gallbladder is disconnected from its attachments and removed.

The procedure is performed under general anaesthesia. While each case has unique characteristics, It generally takes about 30 to 40 minutes for the procedure. Most of the patients can go home in 1 to 2 days.
Because of our extensive experience in laparoscopic surgery, number of stones, size of the stones, size of the gallbladder, presence of acute cholecystitis etc. do not influence the decision against laparoscopic cholecystectomy. Even excessive obesity, in our hands, does not go against laparoscopic procedure. Our specialisations include surgery for weight loss (Laparoscopic Sleeve Gastrectomy and Gastric bypass).
CHOLECYSTECTOMY: MAKING THE DECISION
Once the diagnosis is made, the following facts should be kept in mind:
- It is better to undergo the procedure before any complication (acute cholecystitis, jaundice) has occurred. Presence of complications increases hospital stay and may require additional investigations and procedures thereby adding to discomfort, morbidity and cost. Presence of complications also increases the operating time, chances of conversion to open surgery and prolongs hospital stay and recovery.
- Small/multiple stones have higher potential of slipping out of the gallbladder through the cystic duct into the common bile duct and producing serious complications like jaundice or pancreatitis. They should be treated early.
- If one has diabetes, lives alone, travels frequently or has to travel abroad, it is better to get rid of the disease at the earliest.
- After cholecystectomy, there is no risk of recurrence of gallbladder stones since the organ at fault has been removed.
- Removal of the gallbladder generally leads to no permanent disability or deficiency of the digestive system since in majority of patients, the gallbladder was already non-functioning. In others, the digestion, including that of fatty food, returns back to normal in four-six weeks after which one can enjoy all kinds of food.
- In an otherwise healthy person, laparoscopic cholecystectomy is a safe and simple procedure. While most surgeons use 11 mm instruments for laparoscopic cholecystectomy, we use finer instruments with significantly smaller punctures of three to five mm for this procedure and no stitches are required (sutureless mini/micro laparoscopic cholecystectomy). This saves the patient from apprehension, anxiety and discomfort of suture / clip removal.
EVALUATING YOUR CONDITION
Detailed history and physical examination may help in identifying gallbladder problem and ruling out other causes of pain. Ultrasound has high accuracy (98%) for diagnosing gallstones and associated acute cholecystitis. It may reveal information if stone has passed into the bile duct. Blood tests may also suggest possibility of stone in the common bile duct. Occasionally MRCP, ERCP or CT scan may be required.
In our hands, Laparoscopic cholecystectomy can be safely performed in a large number of patients despite previous (multiple) abdominal operations, second trimester of pregnancy and associated diabetes and heart conditions. With good infrastructure, today there are very few contraindications for laparoscopic surgery.
During laparoscopic cholecystectomy, if at any stage it is felt that it is not safe to continue, the. procedure may be converted to open surgery.
The conversion rate to open surgery varies from center to center and surgeon to surgeon. Important factors influencing conversion rate are experience and skill of the surgeon and quality of the instruments.
Accepted conversion rate is about two or five percent. Conversion in hands of our team is less than 0.25 percent and is generally limited to patients having pus in the gallbladder, multiple previous surgeries or when lung/cardiac condition during surgery prompts conversion to open surgery. In case of conversion, gallbladder is removed through the smallest possible incision.
WHAT ARE THE RISKS AND COMPLICATIONS
Risks and Complications:
Any gallbladder surgery has risks and complications.
These include:
- Excessive bleeding
- Infection
- Injury to abdominal organs
- Injury to common bile duct
- General anaesthesia carries little more risk in patients with diseases of the heart, lungs, kidneys and other systemic problems.
Each Center and each surgeon has a complication rate different from others.
Dr. Kriplani’s large experience of laparoscopic surgery and excellent infrastructure of anaesthesia make the procedure safer and simpler in our setup. In around 12,000 laparoscopic cholecystectomies, technical complications have been encountered in only 0.1% of our patients. There has been no technical complication in our last 5000 patients. We have even removed gallbladder laparoscopically in patients on whom cholecystectomy was attempted else where earlier and part or whole of the gallbladder was left behind due to technical difficulties
IS THERE ANY PROBLEM OF DIGESTION OF FOOD IF THE GALLBLADDER IS REMOVED?
Since the gallbladder is already infected, has decreased capacity (due to stones and shrinkage) and is often non-functioning, the digestion is not adversely affected by Gallbladder removal. Gall bladder does not form bile. It only stores a small amount of bile. Bile production by the liver goes normally after gall bladder removal and the surrounding organs adjust to take over the function of the gall bladder.
Since the gallbladder is only responsible for storage of bile, the production of bile from the liver is unaffected by this operation. Hence, the digestion of food remains normal even after surgery.
WHAT WILL BE MY DIET AFTER GALLBLADDER REMOVAL?
Patients can lead a perfectly normal life without a gall bladder. In fact, most patients report feeling better after surgery and being able to return to their normal life (activity and food) within a few weeks. The digestive system accommodates for loss of gall bladder during this time.
Benefits of laparoscopic surgery:
The benefits of laparoscopic procedure over open surgery are impressive. By decreasing injury to skin and muscles, the resultant pain and discomfort are reduced. Oral intake can be started by the same evening. Most of the patients can be discharged from the hospital the next day as compared to three to five days after open surgery. After laparoscopic cholecystectomy, recovery time (at home) is usually around five days as compared to three-six weeks for open surgery. Tiny punctures of laparoscopic surgery are cosmetically superior to long scar of conventional surgery
Single Incision Laparoscopic Surgery(SILS)
What is SILS?
SILS stands for Single Incision Laparoscopic Surgery. In SILS, only one 12 mm cut is made and the entire surgery is performed through this single small cut. This 12 mm cut is made inside the belly button and is not even visible (scarless surgery). In some patients, another small five mm cut may be required in the upper part of the tummy. Very specialised instruments are used to perform Single Incision Lap Chole and also higher skill and precision are required to perform SILS as safely as the four port technique.
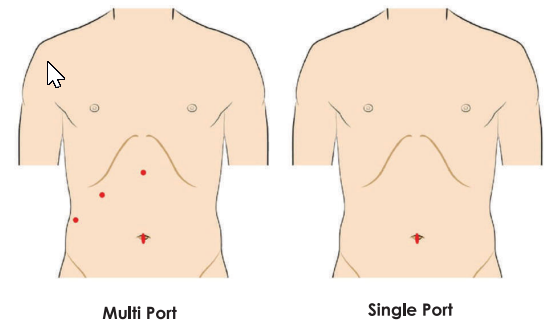

Single Incision lap chole.
Cut completely hidden inside belly button. No visible scar.

Two ports Lap chole.
Note the excellent cosmetic results.
WHY WE NEED TO IMPROVE ON MULTI PORT SURGERY?
Each of these 4 cuts leaves a scar. These 4 scars, though small, adversely affect cosmesis, particularly in females. Also each cut causes some pain. In particular, cuts on the upper part of the tummy are made in muscles and cause more pain.
WHAT ARE THE ADVANTAGES OF SILS?
- The 12 mm cut is completely hidden inside the belly button and is not visible, significantly improving the cosmetic outcome.
- The size of the cuts is one third: from two 11 mm and two six mm ports, it is one 12 mm (and sometimes one six mm) port. Cuts made in the fleshy part of the tummy are avoided and therefore there is significant reduction in pain with faster recovery.
- The tiny cut does not require any stitch and is approximated with a special glue. There are no marks of a stitch and it saves you from subsequent discomfort of stitch removal.
- In the four port technique, four or more titanium (metal) clips are used for clipping the duct and the artery of the gall bladder. If CT scan, MRI, X-ray etc is required in future, the clips will interfere by causing artefacts. In SILS, with our technique no metal clips are used and subsequent CT/MRI can be done without any interference or disadvantage.
We make only one 12mm cut in the belly button and therefore, there is no increased chance for hernia formation in our technique.
IS SILS APPLICABLE IN ALL CASES?
SILS requires tremendous experience and skill to perform the surgery safely. Our team has perfected the technique and we perform more than 95% of our Gall bladder surgeries by SILS. It may not be suitable for patients who have acute infection or pus in the gall bladder, small contracted or thickwalled gall bladder, jaundice, long standing disease, repeated attacks of pain, previous surgery etc. In such situations, (about 5 %), standard four ports may be required to perform lap chole.
WHY SILS IS NOT PRACTICED COMMONLY IN ALL CENTERS?
SILS requires experience and special skills to handle multiple instruments through Single incision which is not easy to acquire. It also requires special inventory of instruments with maintenance cost. Without specialised training and skills it is difficult to perform SILS Chole. We at Fortis Memorial Research Institute, Gurgaon, are doing highest number of SILS Cholecystectomy in the country.
IS SILS A UNIFORM TECHNIQUE?
SILS is done in many different ways. The most commonly practiced way is to make a 25mm cut in the skin and fascia. This however, increases the risk of subsequent hernia formation. We use a hybrid technique which has been developed by us and is novel to our team. This technique needs only a 12mm cut with no increased risk of hernia formation and causes significantly less pain. Ours is a superior technique than the SILS port technique used by others.
WHAT ARE THE PRECAUTIONS?
Belly button should be cleaned thoroughly with soap and water using finger for two-three days before surgery to remove any dirt or concretions.
Hernia
What is Hernia?
WHAT IS THE STORY BEHIND A HERNIA?
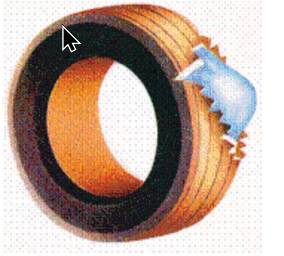
Imagine an old tyre. Its thick wall is like the layers of muscles surrounding the abdomen. The tube inside is the lining of the abdomen from within (peritoneum). Instead of holding air, the abdomen holds various organs & intestines. Usually, the outer wall is strong and keeps its contents in place. Suppose there is a weakness or break in this wall (muscles), the contents tend to come out. In the case of hernia, it is the intestines coming out forming a swelling.
Prompt surgery is recommended for adults as the hernia never goes by itself and keeps growing as the weakness keeps increasing. In advanced cases, hernia can cause serious intestinal and digestive problems and may lead to life-threatening complications.
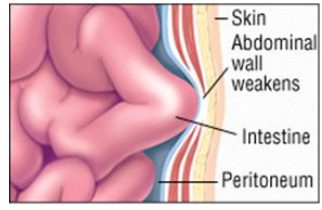
HOW DOES A HERNIA DEVELOP?
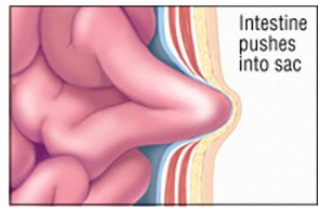
- The wall weakens or tears: A loop of intestine or fatty tissue may push against the inner lining forming a sac. There is no immediate danger at this point, there may not be a bulge or swelling but some burning or tingling might be present.
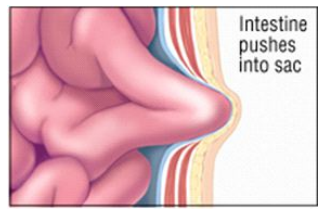
- The intestine pushes into the sac: Most hernias form a bulge as the intestine pushes into the sac. Initially, the bulge flattens out on lying down or pushing against it. This is a reducible hernia. Although there is no immediate danger, prompt hernia repair is required.
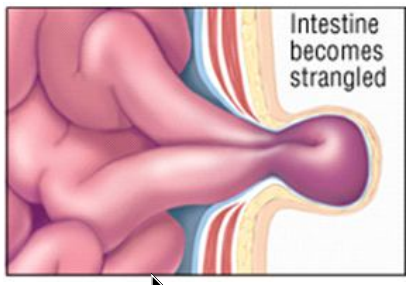
- The intestine may become trapped: If the intestine is trapped, or incarcerated, the bulge cannot be flattened. This is a non-reducible hernia, which is often painful. Urgent surgery is required.
- The intestine may be strangulated: If the intestine is tightly trapped, or strangulated, it eventually loses its blood supply and dies (gangrene). A strangulated intestine can also block digestion and cause severe pain. Emergency surgery is required within a few hours to save life.
Possible weakness = possible Hernia
The abdominal wall contains area of weakness. These area include natural spaces and thin tissue such as the umbilical ring (around navel), internal ring (in groin). Hernias may develop at these or other areas due to ageing, old incision, injury or weakness present at birth. Prompt surgery is recommended for adults as the hernia never goes by itself and keeps growing as the weakness keeps increasing.
What are the Symptoms?
It is easy to recognize a hernia as a bulge under the skin. It may cause pain while lifting heavy objects, coughing, straining during urination or bowel movements. The pain may be sharp and immediate. In some cases, the pain may be a dull ache that gets worse toward the end of the day or after standing for long period of time. In the initial stage, hernia disappears on lying down or by pushing it into the abdomen. Slowly hernia increases in size and becomes increasingly difficult to reduce (incarcerated hernia) causing pain. At any stage, the hernia may get strangulated causing severe pain at the local site, the swelling becomes hard and does not go back into the abdomen and the patient may have vomiting and inability to pass gas (Strangulated hernia). This is a surgical emergency and surgery is needed within a few hours to save life.
Hernia is diagnosed by physical examination and no tests are necessary to diagnose hernia.
What are the treatment options?
Once the diagnosis is confirmed, repair of hernia is the only way to cure it. There is no other treatment available. The weak area needs to be strengthened to prevent the bulge and life threatening complications. Use of truss is cumbersome and will further weaken the muscles by pressure and after some time can be dangerous. It is, therefore, not recommended.
There are three types of surgical hernia repairs: open, minimally invasive and robotic surgery.
Open Surgery: An incision is made over the hernia and protruding organs (mostly small intestine) are pushed back into the abdomen. The weakened area is sewn up and reinforced with a mesh. After surgery, it takes several weeks to fully resume normal activities.
Minimally Invasive Surgery: Through a small incision in the abdomen, a thin laparoscope is inserted with a tiny camera at the end of it. The surgeon and the team can watch the inside of the abdomen on a TV monitor. Under the guidance of the camera, a few other laparoscopic instruments are placed. The hernia is repaired using a mesh. After minimally invasive surgery, there is less scarring, pain and discomfort than open surgery. Patients may also be able to return more quickly to their normal activities.
Robotic Minimally Invasive Surgery: Is the latest technological advance where the surgeon guides and commands a robot to perform the surgery. Robotic surgery is more precise and is supposed to further decrease pain and discomfort than laparoscopic surgery.
Making the decision.
- Once formed, hernia will never go away by itself.
- When the hernia ring is small, chances of a loop of intestine getting obstructed are higher. In fact, 50% of obstructions occur in the first six to nine months of appearance of hernia.
- With passage of time, hernia increases in size by stretching the hernia ring and making the defect bigger. Muscles around the ring become weaker. Therefore larger hernias require larger mesh and repair in larger hernias is not as strong as smaller hernia, with higher chances of recurrence.
- If intestinal loops remain in hernia for a long time, adhesions form (non- reducible hernia). Such hernias are more difficult to repair by laparoscopy, take longer operating time and sometimes may need open surgery.
- If an emergency arises (obstruction/strangulation), surgery is required within a few hours and open repair is the only option. In emergency, the risk of surgery is increased manifold and the quality of repair is less satisfactory since the aim is to save life. Chances of infection and recurrence are higher with emergency surgery.
Repair of larger hernias is associated with increased operating time, more post operative pain, longer discomfort and higher complication rates (seroma, haematoma, funiculitis and hydrocele). The recovery also takes longer.
Once the diagnosis is confirmed, repair of hernia is the only way to cure it. There is no other treatment available. The weak area needs to be strengthened to prevent the bulge and life threatening complications. Use of truss is cumbersome and will further weaken the muscles by pressure and after some time can be dangerous. It is, therefore, not recommended.
There are three types of surgical hernia repair: open, minimally invasive and robotic surgery.
Open Surgery: An incision over the hernia, and protruding tissues are pushed back into the abdomen. The weakened area is sewn up and re enforced with a mesh. After surgery, it takes several weeks to fully resume normal activities.
Minimally Invasive Surgery: Through a small incision in the abdomen a thin laparoscope is inserted with a tiny camera at the end of it. Under the guidance of the camera a few other laparoscopic instruments are placed. The hernia is repaired using a mesh. After minimally invasive surgery, there is less scarring, pain and discomfort than open surgery. Patients may also be able to return more quickly to their normal activities.
Robotic Minimally Invasive Surgery: Is the latest technological advance where the surgeon guides and commands a robot to perform the surgery. Robotic surgery is more precise and is supposed to further decrease pain and discomfort over laparoscopic surgery.
Making the decision.
Once formed, hernia will never go away by itself. However
- When the hernia ring is small, chances of a loop of intestine getting obstructed are higher. In fact, 50% of obstructions occur in the first six to nine months of appearance of hernia.
- With passage of time, hernia increases in size by stretching the hernia ring and making the defect bigger. Muscles around the ring become weaker. Therefore larger hernias require larger mesh and repair in larger hernias is not as strong as smaller hernia.
- If intestinal loops remain in hernia for a long time, adhesions form (non- reducible hernia). Such hernias are more difficult to repair by laparoscopy, take longer operating time and sometimes may need open surgery.
- If an emergency arises (obstruction/strangulation), surgery is required within a few hours and open repair is the only option. In emergency, the risk of surgery is increased manifold and the quality of repair is less satisfactory since the aim is to save life. Chances of infection and recurrence are higher with emergency surgery.
- The likelihood of post-surgery complications like seroma (fluid collection), hematoma (blood) and recurrence are higher for larger hernias and recovery also takes longer. It is therefore wiser to get the hernia repaired when it is small and before complications arise.
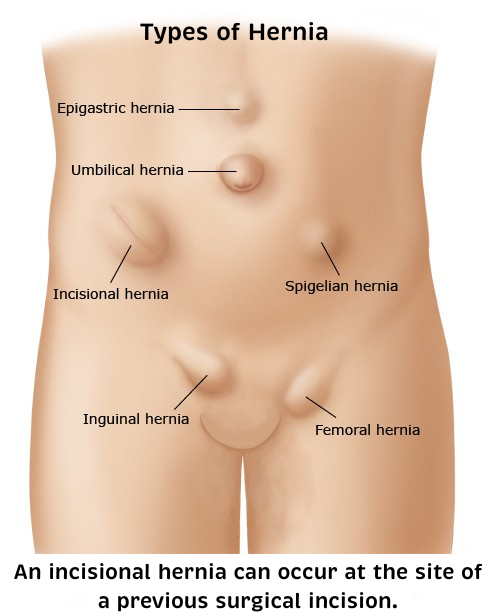
What is Ventral (Umbilical, Epigastric, Incisional) Hernia?
Groin Hernia
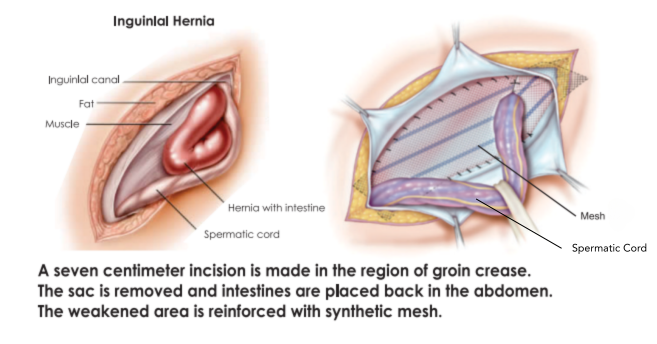
What is Inguinal (Groin) Hernia?
Indirect inguinal hernia is the most common type. It results from weakness at the internal ring where the testicles pass down from the abdominal cavity to the scrotum. In men, it can extend into the scrotum. Direct inguinal hernias are more common in men after the age of 40. They result from a weakness that develops in the muscles of the groin area. Direct hernia often presents on both sides. Inguinal hernia is less common in females.
Bilateral Hernia occurs in about 30% of the patients. A subclinical hernia may be found on the opposite side during office examination. Sometimes, a small hernia on the opposite side is seen only during laparoscopy. If not repaired, it may bulge and require surgery after a few years.
HOW IS OPEN SURGERY FOR INGUINAL HERNIA PERFORMED?
In an otherwise healthy person, present-day inguinal hernia surgery under general anesthesia is safe. However, in patients with severe heart disease, asthma, and kidney damage etc., general anesthesia may not be safe and in such situation safer choice (local/spinal anesthesia) can permit open surgery for inguinal hernia with acceptable risk.
Discharge from the hospital is usually after 24 hours. After 10 – 14 days of rest, one can start outdoor activities and return to normal routine over three-four weeks. Lifting heavy objects and strenuous exercises should be avoided for three to four months.
HOW IS LAPAROSCOPIC INGUINAL (GROIN) HERNIA REPAIR PERFORMED?
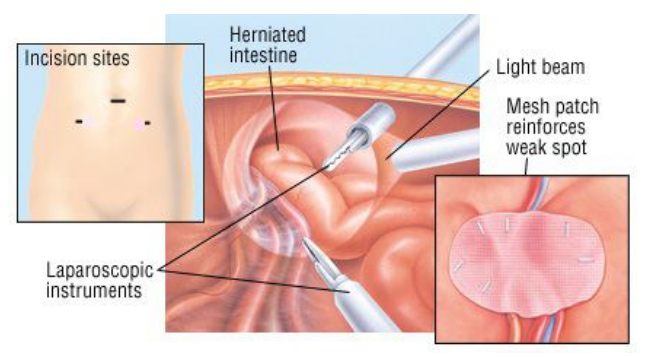
Laparoscopic surgery allows the surgeon to see clearly into the abdomen and to repair the hernia from inside. The laparoscope, a tiny “telescope” attached to a camera, gives a close-up view of the hernia. Since laparoscopic surgery doesn’t require large incisions, it is less painful than open surgery and results in a faster recovery. The pain is also less because the cuts are made on the immobile and less sensitive skin of the abdomen. Usually, the surgery takes 40-45 minutes for one-sided inguinal hernia. One can go home the next day and return to normal activity in about a week.
Tiny Incisions
- The procedure is performed under general anesthesia to ensure that the patient sleeps without pain throughout the procedure. Generally, three or four ports are made. One 10 mm puncture is made near the navel (for the telescope) and two 5 mm ports on either side of the navel for instruments.
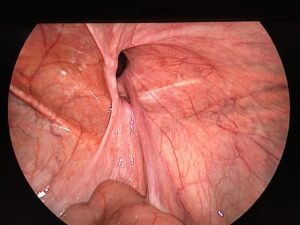
The View from Inside
- A powerful light beam shines inside the abdomen, allowing the surgeon to see the hernia. The tiny video camera on one end of the laparoscope projects a clear picture of the inside of the abdomen onto a video monitor, providing a magnified view for precise and accurate repair.

- The surgeon places the intestine or other tissues back inside the abdomen. Then, the area of weakness in the abdominal wall (hernia ring) is exposed by dissecting the peritoneum over it. The hernia sac is reduced.
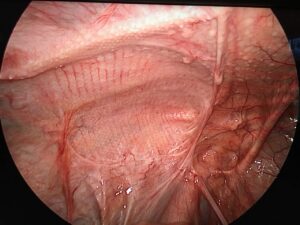
Reinforcing the Weakness
- A high-quality synthetic mesh is placed directly over the weakened area (hernia ring) to widely overlap the defect. The mesh is fixed in place with surgical staples (tensionless repair). It remains in place permanently, incorporating into body tissues over time to ensure a strong repair.
- The mesh is covered by the peritoneum again, and carbon dioxide is released from the abdomen. The skin incisions are approximated.
HOW IS LAPAROSCOPIC REPAIR DIFFERENT FROM OPEN REPAIR?
- The most important aim of hernia repair is to eliminate recurrence.
- Recurrence rates for open inguinal hernia repair are 1%-5% worldwide. However, laparoscopic repair uses a larger mesh (16×12 cm, compared to 12×5 cm for open repair). This provides stronger repair with wider defect overlap. Recurrence rate in our hands is almost zero
There is significate reduction in post operative pain after laparoscopic than open repair, which becomes further significant after bilateral repairs. Returning to work, driving, sports, and exercise is quicker and less painful after laparoscopic repair (7 to 10 days versus 3 to 4 weeks after open repair), due to the larger mesh size and smaller incisions.
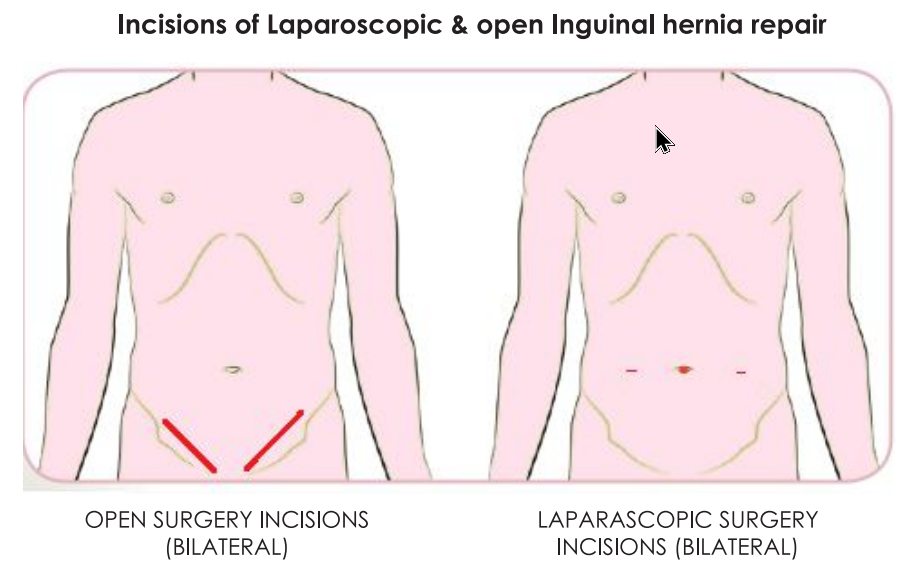
- While with the laparoscopic approach, simultaneous repair of both-sided hernias can be performed, the open approach requires staged procedures, with repair of only one side at a time.
- After conventional hernia repairs, some feeling of numbness of the skin below the cut is not uncommon, as small nerves supplying the skin are inadvertently cut during surgery. In laparoscopic repair, no such damage is done since cuts are small.
- However, laparoscopic hernia repair is a demanding technique for the surgeon. The surgery requires a thorough understanding of anatomy, as well as experience and skill to produce good results. It is difficult to handle a large piece of mesh during laparoscopic surgery without expertise. The mesh must be placed very precisely with equal overlap on all sides of the hernia ring.
WHAT IS ROBOTIC INGUINAL HERNIA REPAIR?
Robotic platform allows the surgeon to do a more precise surgery by a magnified 3D view. Robotic instruments have more manoeuverability. The use of stapler, which causes pain, is discouraged. The mesh and the peritoneum are sutured . This results in further reduction in the post operative pain and early mobility. The use of robotic surgery has seen a rapid upsurge in the field of surgery, particularly hernia surgery.
WHAT ARE THE PRECAUTIONS TO BE TAKEN BEFORE SURGERY?
- Your general health will be checked with blood and other tests. An anesthesiologist will review your reports and conduct a physical examination.
- Avoid blood-thinning medications (aspirin, clopidogrel) for five days before surgery.
- Stop smoking a few weeks before surgery to prevent complications from “smoker’s cough” and to ensure better healing. Smokers can have breathing problems during and after surgery, which can put pressure on the repair. Smoking also negatively affects healing process.
- Inform if you consume tobacco. In long-term tobacco users, the intestine becomes dependent on nicotine and post surgery they are likely to have abdominal distension. Such patients need extra monitoring and management.
- If you are grossly overweight (BMI more than 30 Kg/m2), losing some weight before surgery will improve your outcome. In obese patients, the incidence of recurrence is higher, as fat weakens the muscles.
- In diabetic patients, blood sugar and HbA1C must be within expected range as chances of infection are higher in uncontrolled diabetics and healing becomes poor.
- Sleep apnea is a common breathing problem. If you have sleep apnea, you stop breathing for short lengths of time while you’re asleep. The most common type is obstructive sleep apnea (OSA). With OSA, your airway becomes fully blocked during sleep. OSA can cause serious problems during and after surgery. Tell us if you have or think you might have sleep apnea. If you use a breathing device, such as a CPAP machine, bring it on the day of your surgery.
- Clean the navel thoroughly with soap and water for 2-3 days before surgery to remove any dirt or debris.
WHAT TO EXPECT POST-SURGERY?
- After surgery, you will be monitored in the recovery room. The decision to shift you to your room depends on the anesthesiologist’s assessment.
- Nausea or vomiting may occur in the first few hours but will subside with deep breathing, sitting upright and moving toes.
- Small strips will cover your incisions. Any discomfort in your right shoulder is temporary and should resolve in a few days.
- Movement is encouraged within a few hours to promote circulation and reduce pain.
- Tightness and bloating in the abdomen are normal due to the dressing supporting the mesh. Swelling over the hernia site (seroma) is common and will subside within a few weeks.
WHAT ARE THE PRECAUTIONS TO BE TAKEN THE DAY AFTER SURGERY?
- You can have normal breakfast in the morning and semisolid food in the day (khichri, porridge, toast, biscuits, and cookies). Some bloating of abdomen may be present which will disappear after regular passage of wind and stools. Since nothing much was taken by mouth the day before, one generally does not pass stools and hence, should not strain.
- You will be discharged on the next day of operation after groin hernia repair, unless there is some medical/social reason. You can walk normally and can climb stairs slowly. Ventral hernia patients may have to stay for two to three days depending on the size and complexity of hernia.
- As the mesh is non-stretchable, some patients may have a feeling of stiffness and tightness over the hernia site for a few days. It is more commonly felt when repair is done on both sides and after ventral / incisional hernia.
HOW DO I LOOK AFTER MYSELF AT HOME?
After 48 hours, groin hernia patients can start taking normal diet, shower and can walk at home. Water can flow over the dressing but do not rub over it. The dressings do not need any change. If they come off, they do not need any replacement. If they do not come off, they will be removed during hospital visit. One can start going outdoor in five days and return to normal activity as soon as possible.
Scrotal support should be worn for three to four weeks after groin hernia repair. The bigger the hernia, the longer the duration of scrotal support.
Ventral hernia patients are applied tight dressing which stays for 4-5 days. They can not have bath till that time. After 5 days the dressing is removed and abdominal support belt applied. They can then have a bath.
Hernia support belt must be worn for two to three months after ventral / incisional hernia repair (24 hours for first month & during daytime for next two months).
In some situations, particularly with direct hernias, large hernias or overweight patients, some fluid may collect in the empty space left by the hernia (seroma). It can be avoided by properly wearing hernia support belt / scrotal support. It will go away in ten to twelve weeks. Some skin discoloration (called ecchymosis) may be noticed around the hernia site. It will disappear over a few weeks.
You should fix up an appointment with our team after 7 – 10 days. Call earlier if you have any significant problem like fever, redness, increasing pain, excessive swelling (some swelling is common), vomiting, blotting, etc. After removing the dressing, apply skin cream on the cuts twice a day for five days. Please do not scratch over the scabs or pull them out. They will fall off eventually.
One may start going to work in 7-10 days. Avoid long working hours and fatigue in the first few days. Your body should decide how much to work. Outstation patients can leave Delhi after five days. Driving four-wheelers can be resumed after 7-10 days. Business traveling can be resumed after 10-14 days.
As the mesh is non-stretchable, some patients may have a feeling of stiffness and tightness over the hernia site for a few days. It is more commonly felt after bilateral groin hernia or larger ventral hernia.
Ventral Hernia
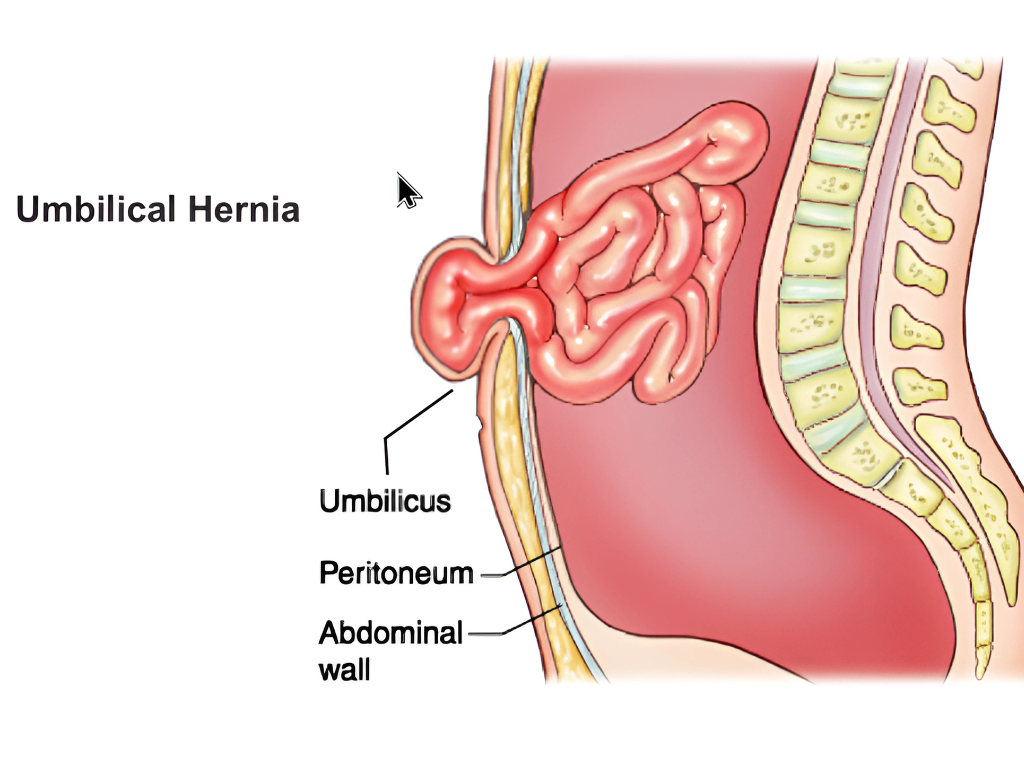
What is Ventral (Umbilical, Epigastric, Incisional) Hernia?
- Umbilical Hernia:
An umbilical hernia looks like an inflated or bulging navel. It is caused by a weakness that may be present at birth or is acquired over time. Children and adults of both genders can develop an umbilical hernia. - Epigastric Hernia:
An epigastric hernia appears in the midline between the breast bone and belly button due to weakness of tissues. The fat pushes through a weakened area in the abdominal wall, forming a lump. Small hernia may not cause any symptom, but larger ones can cause pain and may require surgery. Some patients develop more than one epigastric hernia at a time. - Incisional Hernia:
A hernia that occurs in the area of a previous surgery is known as an incisional hernia. Incisional hernias are relatively common because surgical incisions weaken the abdominal area. That weakness makes it easier for a part of the intestine or other tissue to protrude. Incisional hernias can develop soon after surgery, or they can develop slowly, over months or even years. Incisional hernias tend to be large and rather painful. Incisional hernias need surgery because they may enlarge and become increasingly difficult to repair.

Increased abdominal pressure due to obesity, excessive coughing or pregnancy may predispose to umbilical or incisional hernia.
HOW IS THE OPEN SURGERY FOR VENTRAL HERNIA PERFORMED?

Umbilical and Incisional hernias are generally repaired under general anesthesia.
Reinforcement: The incision of the earlier surgery is reopened along its entire length. The intestine is placed back into the abdominal cavity. The hernia defect is closed by pulling together and suturing the abdominal tissue or reinforcing it with a synthetic mesh.
One or two drainage tubes are placed under the skin at the end of surgery to prevent fluid collection. These are removed when they stop draining fluid, typically in 4-5 days, though it may take longer in overweight patients. Oral fluids are generally started 24 hours after smaller hernia surgeries and 48-72 hours for larger hernias. Stitches are typically removed after 10-14 days.
After discharge from the hospital, rest for 10-12 weeks is required at home, before resuming a normal routine. One should wear an abdominal binder for three months after surgery.
Open surgery for incisional or moderate-size umbilical hernias involves significant pain and discomfort due to the large incision. Wound issues like skin gaping, seroma (fluid collection), and infections may occur. A recurrence rate of 5-10% is acceptable. In long-standing umbilical hernia cases, the navel skin becomes excessively stretched and thinned. The belly button may need removal during open surgery.
HOW IS LAPAROSCOPIC VENTRAL HERNIA REPAIR PERFORMED?
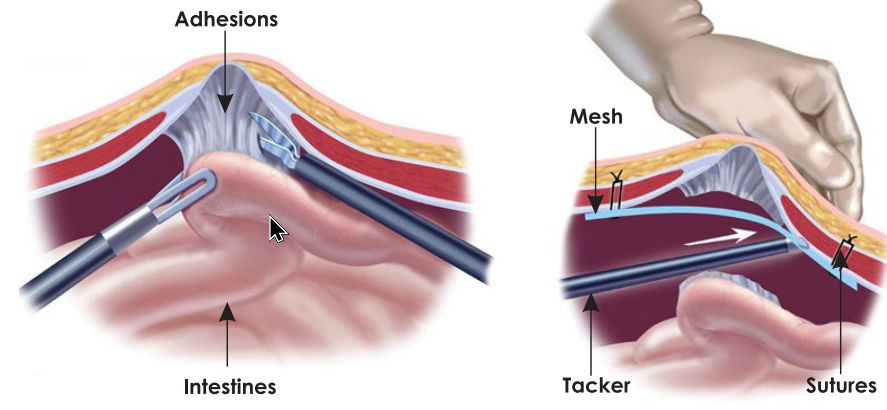
- The repair is performed under general anesthesia. Carbon dioxide is injected into the abdomen to distend it, creating space for the laparoscopic instruments.
- Three to four tiny punctures (5 – 10 mm) are made. A laparoscope and instruments are inserted through these incisions. For incisional hernias, all punctures may be on the left side.
- A powerful light beam inside the abdomen and a video camera provide a magnified view.
- The surgeon places the intestine back inside the abdomen and exposes the weak abdominal wall area (hernia ring).
- A strong synthetic mesh is placed over the weak area to widely overlap the defect. It is secured with surgical staples and sutures.
- Carbon dioxide is released, and skin incisions are closed.
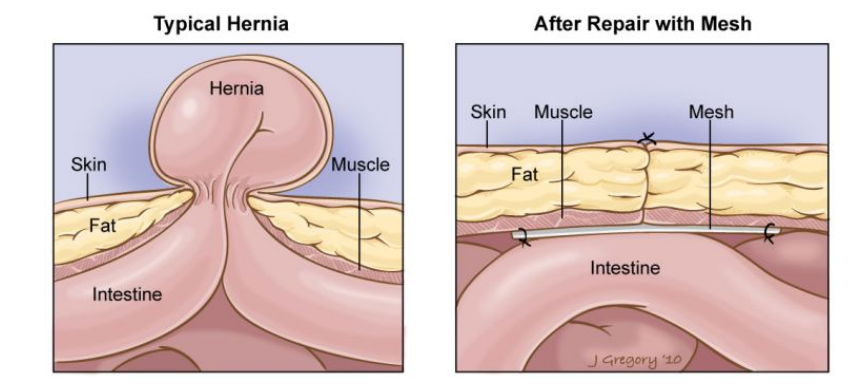
WHAT ARE THE ADVANTAGES OF LAPAROSCOPIC VENTRAL HERNIA REPAIR?
- Small wounds (punctures) instead of large incisions.
- Significantly less pain.
- Low incidence of seroma (fluid collection).
- No need for drainage tubes as usually applied in open repair.
- Early resumption of diet as intestines are not disturbed.
- Shorter hospital stay with minimal chances of infection.
- Faster recovery and return to daily activities.
- Almost zero recurrence (in our experience).
- Wound complication (breakdown, sepsis, necrosis) minimized making recovery faster.
- Superior cosmetic results. The navel skin, which is often removed in open repair, is preserved in laparoscopic repair.
HOW IS OUR TECHNIQUE OF LAPAROSCOPIC VENTRAL HERNIA DIFFERENT?
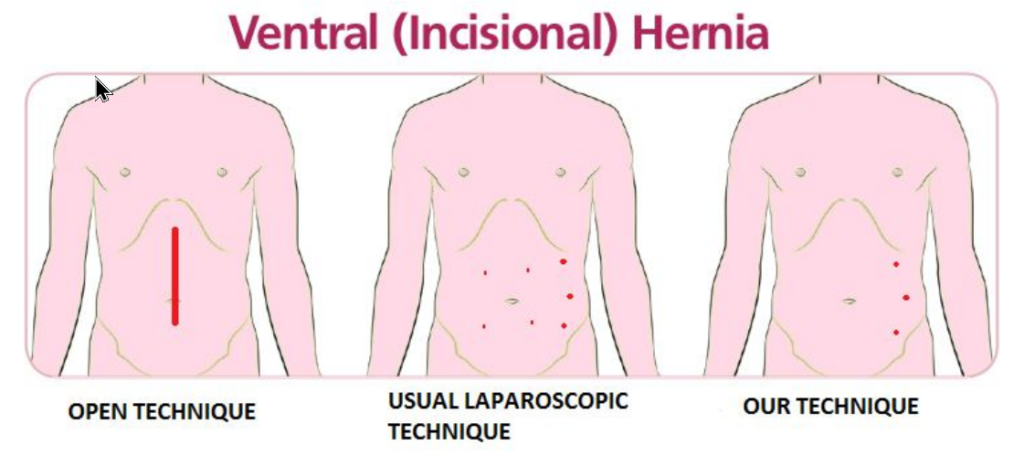
- Only three tiny punctures are used: one 10 mm and two 5 mm (compared to larger or more incisions by others).
- No additional punctures over the anterior abdominal wall (others make extra punctures for mesh fixation, causing scars and pain).
- We put wide intra-corporeal (totally inside) stitches to fix mesh which is many times stronger than trans-facial stitches and cause less pain [exclusive to us & very difficult to replicate as it is technically challenging]
WHAT IS ABDOMINAL WALL RECONSTRUCTION FOR VENTRAL HERNIA?
In laparoscopic hernia repair, the defect in the abdominal wall is bridged by placing a mesh and fixing it in place when the abdomen is distended with pneumoperitoneum. This may leave a lax abdominal wall and the mesh bulging through the defect causing a pseudo hernia resulting a protruding abdomen. In long term, the mesh may get displaced permanently resulting in recurrence in about 5% to 8% of patients.
Abdominal Wall Reconstruction is a specialized technique for superior outcome of ventral hernias including large / recurrent hernia. In this procedure, the defect in the abdominal wall is closed by sutures (reconstruction of the linea alba) and may require mobilization of the components of the abdominal wall to relieve the tension on the tissues (tension less repair). A very large mesh is then placed to reinforce the tissue repair. This makes a dynamic, functional abdominal wall with superior cosmetic outcome and decreased recurrence.
WHAT IS ROBOTIC VENTRAL HERNIA REPAIR?
Robotic platform is a cutting edge technology, which allows the surgeon to do a more precise surgery by a magnified 3D view. Robotic instruments have more manoeuverability. The use of stapler, which causes pain, is minimised and the mesh and peritoneum are dominantly sutured with resultant further reduction in the postoperative pain and early mobility. The use of robotic surgery has seen a rapid upsurge in the field of surgery.